Retake
N5) Altered mental status after fall with head injury
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with altered mental status.
- Review the DDx considerations in a patient with altered mental status.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with altered mental status.
History
A 70-year-old male with a history of alcoholism and multiple falls presents to the emergency department following a recent tonic-clonic seizure, which occurred approximately 30 minutes after a fall with a head strike. The seizure was accompanied by subsequent nausea and vomiting. According to the patient's spouse, he has experienced difficulty moving his left arm and leg and has displayed signs of confusion over the past day.
Physical Exam
BP: 160/100 mmHg, HR: 60 bpm, RR: 10 breaths per minute, Temp: 37°C (98.6°F), O2 saturation: 96%.
Pulmonary: Cycles of progressively deeper and faster breaths followed by apnea.
Neurologic: 3+ deep tendon reflexes, decreased sensation, and 4/5 strength in the left upper and left lower extremities. Right pupil fixed and dilated. GCS 10
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient’s presentation, including focal neurologic deficits, altered mental status, new onset seizures after a fall, and other accompanying signs, strongly suggest a intracranial hematoma. The presence of a right-sided blown pupil, contralateral motor deficits, Cushing's triad (hypertension, bradycardia, and Cheyne-Stokes respirations), and nausea and vomiting suggest that this condition has led to brain herniation.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires emergent workup and intervention considering the suspected brain herniation.
First Imaging Study
What is the first imaging study you will order?
Given the patient's moderate Glasgow Coma Scale (GCS) score after acute head trauma, a CT head without IV contrast is most appropriate because it is effective in detecting lesions potentially requiring neurosurgical intervention such as hemorrhage, herniation, and hydrocephalus, and provides predictive value regarding outcomes and management needs in traumatic brain injury patients. Contrast should not be administered to evaluate blood.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
CT head without contrast
What type of intracranial hemorrhage is present?
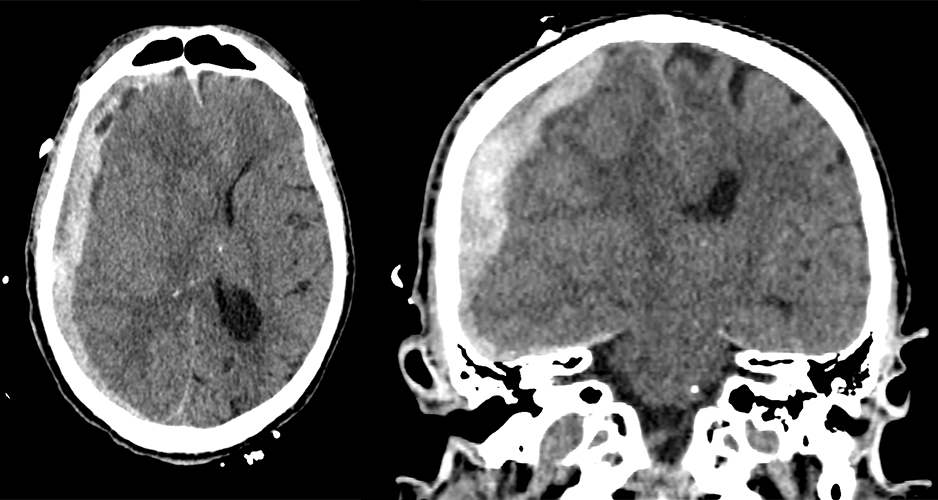
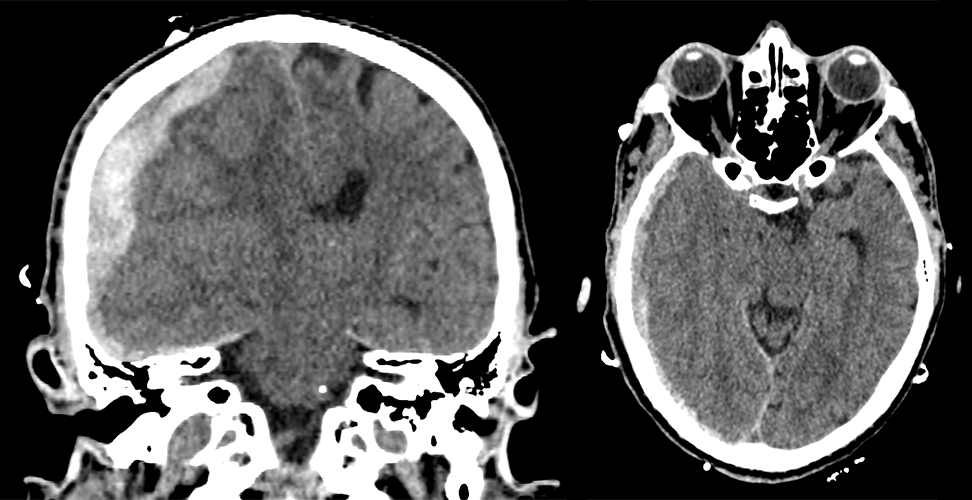
A subdural hematoma is often crescent-shaped on imaging and can cross suture lines, typically resulting from trauma that damages the bridging veins. An epidural hematoma is usually lens-shaped and doesn't cross suture lines, commonly due to a skull fracture that injures an artery. A subarachnoid hemorrhage represents bleeding in the subarachnoid space, with blood visible in cisterns and sulci, often due to a ruptured cerebral aneurysm or trauma. A hemorrhagic contusion is essentially a brain bruise, with blood accumulating in brain tissue (intraparenchymal), usually seen after high-impact trauma.
There is evidence of herniation.
The intracranial hemorrhage leads to right uncal herniation and right subfalcine herniation.
There is midline shift.
There is right to left midline shift secondary to the right sided hematoma.
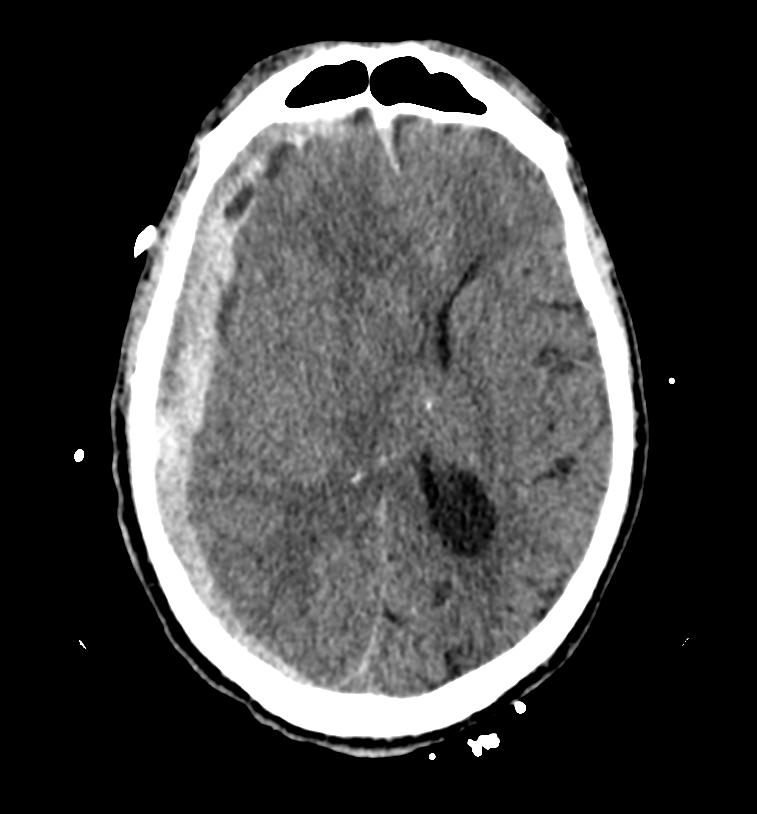
The hypodensities within the bleeding hemorrhage represent:
Hyperacute appears hypodense on CT imaging. This is due to the fact that it's still in a liquid state with unclotted red blood cells. In contrast, acute blood (hours to 1-2 days old) and subacute blood (2-3 days to several weeks old) usually appear hyperdense (bright) as the blood begins to clot and reorganize. Chronic blood (weeks to months old) appears hypodense again, as it's in the stage of hemosiderin deposition and the breakdown and resorption of blood products.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is necessary as the diagnosis is confirmed with the CT scan.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
Generally, a midline shift of greater than 5mm and subdural hematoma thicker than 10mm are considered thresholds for surgical intervention. Furthermore, this patient also has herniation, focal neurologic deficits, and a lesion secondary to this hematoma, which is actively bleeding.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient with an actively bleeding subdural hematoma leading to herniation and midline shift requires emergent management.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a 70-year-old male with a history of alcoholism and falls, presenting with altered mental status, a blown right pupil, focal neurologic deficits, and a new onset seizure. Imaging revealed an actively bleeding right subdural hematoma causing a 17mm midline shift to the left, as well as right uncal and transtentorial herniation with ventricular entrapment. Neurosurgery should be urgently consulted to evaluate the need for surgical evacuation. The patient should be admitted to the neurological ICU and undergo frequent neurological exams. Antiepileptics should be administered. Consideration should be given to using mannitol or hypertonic saline to manage increased intracranial pressure. The patient should be made nil per os (NPO) in preparation for potential surgery. Additionally, the patient should be monitored for alcohol withdrawal syndrome using the Clinical Institute Withdrawal Assessment (CIWA) scale. Depending on the patient's recovery, involvement of social work may be necessary for alcohol counseling.
Lessons Learned:
- Subdural hematomas are a type of intracranial hemorrhage resulting from traumatic brain injury, characterized by bleeding between the dura and arachnoid mater.
- This type of herniation can lead to life-threatening brain herniation, which can manifest as neurological deficits such as loss of consciousness, motor abnormalities, or cranial nerve dysfunction.
- Subdural hematomas are common in elderly or alcoholic patients who are prone to falling. Increased brain age and alcohol use can lead to cerebral atrophy, increasing the risk of trauma from damage to the bridging cerebral veins.
- A crescent-shaped, concave hematoma that crosses suture lines is indicative of a subdural hematoma.
- Small subdural hematomas that are largely asymptomatic can often be managed conservatively. Hematomas larger than 10mm, hematomas leading to a midline shift of 5mm or more, evidence of herniating structures, and rapid neurologic deterioration generally require surgical intervention.
Socioeconomic Factors: Primary care physicians should evaluate fall risk factors in elderly patients.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}